
MCA Territory Infarct Treatment
The middle cerebral artery (MCA) supplies a large proportion of the lateral hemisphere including motor function and the genu of the internal capsule.
Typically MCA infarctions are embolic, with clots travelling from the heart and settling in the artery. The resulting arterial occlusion leads to brain ischemia with secondary effects that depend on the hemisphere affected.
Symptoms
The middle cerebral artery (MCA) is the largest blood vessel in the brain. It provides oxygenated blood to over 80% of the brain. This large distribution means that insufficient blood flow to this area can cause a variety of neurologic deficits. Insufficient blood supply is referred to as ischemic stroke.
Symptoms of a stroke in the MCA territory can vary depending on what part of the brain is affected. The MCA is the main blood supply to the frontal, temporal and parietal lobes, most of the basal ganglia, and parts of the internal capsule and caudate. It also supplies the deep perforating lenticulostriate branches of the MCA which provide blood to the inner structures like the internal capsule.
MCA strokes can be ischaemic or hemorrhagic. Ischaemic strokes are caused by blockage of a blood vessel that impedes the delivery of oxygenated blood to brain cells. Blood vessels can be blocked by clots or by the build-up of plaque or fat deposits. Blood vessels can also rupture, such as in hemorrhagic stroke.
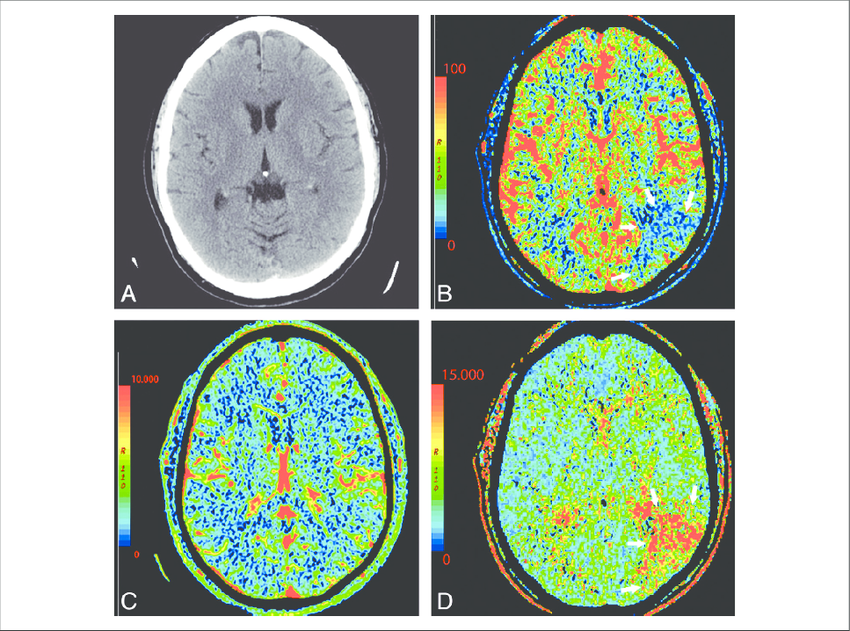
The patient in this case presented with slurred speech without aphasia, right gaze preference with incomplete left hemispatial neglect, and weakness of the left arm and leg (NIHSS score of 12). A brain MRI three days later showed sparing of the precentral gyrus (PCG) and showed a new complete right MCA territory infarct (fig 1B). Echocardiography showed a patent foramen ovale and doppler lower extremity studies did not show deep venous thrombosis.
Diagnosis
The diagnosis of a stroke usually involves a physical exam and imaging tests such as CT or MRI scans. These can help identify symptoms such as weakness or numbness on one side of the body, difficulty speaking, or problems with vision.
The middle cerebral artery (MCA) is part of the Circle of Willis, and it supplies blood to most regions of the brain. A stroke in the MCA territory typically causes movement or sensory deficits on the opposite side of the body, speech difficulties, and trouble swallowing (dysphagia).
Infarctions in the MCA territory are also called penetrating artery strokes because they occur when an embolus pierces the blood vessels in the brain. These are less common than non-penetrating strokes, but they can be just as severe.
Symptoms of MCA strokes vary depending on which divisions or branches are involved and how large the infarct is. If the MCA’s anterior (superior) division is involved, it commonly results in contralateral hemiparesis and hemisensory loss. If the MCA’s lateral Rolandic artery is involved, it typically spares the motor strip in the precentral gyrus (PCG). This sparing of PCG is observed in three cases of large MCA infarctions that show similar clinical and neuroimaging characteristics. The authors hypothesize that spontaneous local recanalisation of the occluded vessel may have selectively restored flow to the PCG, leaving other parts of the ischemic penumbra2 unaffected.
Treatment
A stroke is an ischemic event that results in loss of oxygen to the brain. It is a leading cause of morbidity and mortality in the United States. The middle cerebral artery (MCA) is the blood vessel that supplies most of the outer convexity of the brain, all of the basal ganglia, and part of the anterior and posterior internal capsules. Therefore, if the MCA is occluded it can lead to many different types of neurologic deficits. The MCA is wrapped in a circle of vessels known as the Circle of Willis. This vascular territory is particularly vulnerable to reduction in blood flow and oxygen supply due to its distance from the main arterial arteries.
The MCA is often occluded by clots that form in the perivascular space (the area surrounding the arteries), which is also called the “watershed zone”. When this happens, it can be very difficult to recanalize the infarct. Thrombolysis is the only treatment that has been proven to reopen occluded arteries in the early stages of an MCA stroke. The window of time for receiving this therapy is very short, however.
A 67 year old woman presented to the emergency department in collapse with right gaze preference, left sensory hemi-neglect, and moderate (4/5 proximally) weakness of her left arm. A head CT and brain MRI demonstrated a small old infarct in the left cerebellum as well as a new complete occlusion of the right MCA, with sparing of the PCG. The patient received IV tissue plasminogen activator and underwent mechanical thrombectomy. She was transferred to a rehabilitation facility where she regained her strength and now walks independently with two walking wheelchairs.
Prevention
The MCA is by far the largest blood vessel in the brain and is the blood vessel most commonly affected by stroke. It supplies most of the outer convex brain surface, the entire basal ganglia and nearly all of the internal capsules. Hence, an MCA territory infarct can produce very diverse neurologic deficits.
In the acute setting, IV tissue plasminogen activator (TPA) or thrombectomy may be used, depending on whether the patient qualifies and is within the 4.5 hour window after onset. Treatment beyond this point is focused on symptom management and secondary stroke prevention.
Stroke symptoms are often characterized by weakness or numbness on one side of the body, difficulty swallowing and a speech disturbance. These symptoms are caused by the loss of blood supply to part of the brain, which causes an infarct.

